Cystine Stones: Developments in Minimally Invasive Surgery and Their Impact on Morbidity and Stone Clearance
1Department of Urology, Warwick Hospital, Warwick, UK; 2Department of Urology, Sismanogleio Hospital, National and Kapodistrian University of Athens, Athens, Greece; 3Department of Urology, University Hospital Southampton, Southampton, UK
Correspondence: Bhaskar K Somani, University Hospital Southampton NHS Trust, Southampton, UK, Tel +44-2381206873, Email bhaskarsomani@yahoo.com
Abstract: Cystinuria is a rare genetic condition that is responsible for cystine stones. Besides stone recurrence, patients with cystine stones have reduced health-related quality of life, increased rates of chronic kidney disease and hypertension. Although lifestyle measures, medical therapy and close follow up are essential to reduce and monitor cystine stone recurrences, surgical intervention is frequently needed for most cystinuria patients. Shock wave lithotripsy, ureteroscopy, percutaneous nephrolithotomy and active surveillance all have a role, and technological advances in endourology are vital in achieving a stone-free status and to prevent recurrences. The complexity of managing cystine stones necessitates a multidisciplinary team discussion, patient involvement and an individualised approach in a specialist centre for optimum management. Thulium fibre laser and virtual reality may have an increasing role in the future of cystine stone management.
Keywords: kidney calculi, ureteroscopy, percutaneous nephrolithotomy, laser, cystine, recurrence
Introduction
Cystinuria is a rare genetic condition that is responsible for cystine stones that account for approximately 1% of urolithiasis in adults.1 In the paediatric population cystine stones account for approximately 8% of urinary stones.2 Cystinuria is an inborn error of metabolism inherited as either an autosomal recessive or autosomal dominant, with incomplete penetrance mechanism.3 Cystinuria itself has a global incidence of approximately 1 in 7000 with variability between different patient groups.3
Mutations in the SLC3A1 or SLC7A9 genes result in defects of trans-epithelial transporters in the renal proximal tubules that normally reabsorb cystine, ornithine, lysine and arginine, consequently increasing the urinary concentrations of these amino acids.4 More than 200 mutations have been recognised in these genes and cystinuria can be classified according to whether the defects are within SLC3A1 (type A cystinuria), SLC7A9 (type B cystinuria) or rarely where a mutation arises in both genes (type AB cystinuria).3,5 It is only increased urinary levels of cystine that are of clinical significance due to it being relatively insoluble at physiological urinary pH resulting in precipitation and stone formation. Stone analysis can be used to diagnose cystine stones, or in the absence of a stone, a quantitative 24-hour urinary cystine level.6 Although advances in genetic sequencing have enabled the possibility of identifying the exact mutation present, this is not currently routinely recommended as it does not alter clinical practice.5–7
The genetic nature of the disease typically results in patients with cystinuria developing stones at an earlier age with a greater chance of recurrence than other stone formers.8 The median age at presentation is adolescence, but the rarity of this disease often results in a delayed diagnosis of cystinuria, 7.8 years reported by one UK study.9 Furthermore, patients typically required more surgical treatments than patients with non-cystine stones8 with a systematic review reporting a mean of 5.7 procedures per patient over an average 9.6 year follow up, with a mean of 0.59 surgical procedures/patient/year.10 This cohort will therefore benefit greatly from minimally invasive surgery (MIS) to lessen the impact of morbidity from repeated open surgical procedures.
Patients with cystine stones have reported reduced health-related quality of life (HRQoL) compared with patients with non-cystine stones.11 Cystine stone formers have also been found to have increased rates of chronic kidney disease (CKD) and hypertension.12 Even in the paediatric population, renal scarring is commonplace on DMSA imaging, although this did not correlate with renal impairment.13 Nephrectomy is not uncommon due to the delayed diagnosis, with a rate of 8% of patients having undergone previous nephrectomy in one study.9
Non-Surgical Management
Whilst cystinuria is not curable, except for rarely performed renal transplantation,14 dietary modification and pharmacological management can reduce cystine concentration in the urine and therefore reduce stone formation6 (Figure 1). Fluid intake sufficient to produce a minimum of 3 litres of urine a day in adults has been advocated with the intention of diluting the urinary cystine concentration to <250 mg/L, therefore inhibiting cystine crystallisation.6,15 Restricting consumption of sodium to <2500 mg/day is also recommended as this is associated with reducing urinary cystine excretion.6,16 Reducing consumption of animal protein has also been proposed as this is high in methionine, a precursor of cystine, which will therefore increase urinary cystine excretion. However, children should still meet recommended daily protein intake as this is essential for growth.6,17
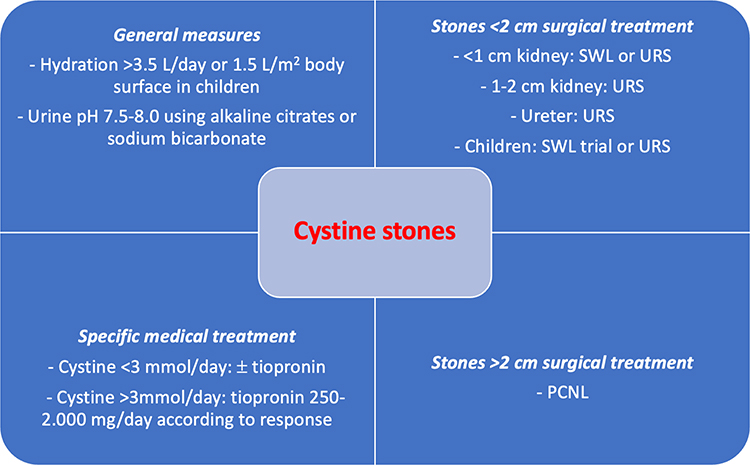 |
Figure 1 Summary of management in patients with kidney stones. Abbreviations: SWL, shock wave lithotripsy; URS, ureteroscopy; PCNL, percutaneous nephrolithotripsy. |
Cystine solubility is strongly affected by urinary pH with physiological urinary pH (5.0–7.0) being associated with the lowest solubility.18 Alkalinisation of urine with potassium citrate can increase the solubility of cystine, with the American Urology Association (AUA) recommending a target pH of 7.0 and the European Association of Urologists (EAU) advocating a target pH of 7.5–8.5.19,20 However, caution should be exercised with alkalinisation of urine as this can increase the risk of calcium phosphate stones.21 Response to treatment can be assessed with measuring urinary pH and 24-hour urine collections with a target of <3 mmol/day of cystine.20 Second-line treatment with cystine binding thiol drugs (CBTD) (e.g. tiopronin preferred over penicillamine due to improved side-effect profile19,22) are indicated if urinary cystine excretion remains >3 mmol/day despite adequate alkalinisation.6,20
Surveillance
The EAU guidelines recommend close follow up of high-risk stone formers, including those with cystinuria, with imaging, metabolic management and treatment monitoring initially at 6 months and then annually.20 However, this should be adapted to individual patient circumstances as frequent stone formers may require regular follow-up and ideally this would be in a specialist clinic.9,23,24
Although X-ray, ultrasound and CT have all been used in active surveillance of cystinuria patients for small asymptomatic stones, ultrasound is often preferred to reduce the cumulative radiation exposure from repeated imaging.15,23,25 Although the EAU recommends at least annual follow up, this may be as frequently as 3-monthly depending on the individual patient and their frequency of stone recurrence.
As with other stone types, a trial of conservative management or medical expulsive therapy and close observation can be considered in obstructing ureteric stones <10 mm with no evidence of fever, infection, renal impairment, or uncontrolled pain.19,23 Thomas et al reported that 53% of their cystinuria patient cohort passed their stones spontaneously and therefore those with small asymptomatic stones may be managed conservatively with appropriate close monitoring, deferring surgical intervention to a point where stones become symptomatic or too large to pass spontaneously.9 Individual patients should be involved in the decision-making process, and patients may have a preference for less invasive procedures due to a history of frequent surgery. An active surveillance strategy with regular follow up including ultrasound (US), as well as radiography from time to time, is a valid option that prevents patients from unnecessary interventions and thus the risk of intervention-related complications.
Despite dietary and pharmacological management to reduce stone formation, surgical management is not uncommon for most cystinuric patients. Developments in minimally invasive surgeries (MIS) have seen a dramatic change in practice for managing cystine stones over the last few decades.26 The purpose of this article is to review the impact of minimally invasive surgery and technical advances on outcomes of recurrent cystine stones.
Surgical Management Options
The need for open surgery to treat upper tract urolithiasis is now largely redundant due to the significant advances in MIS with ureteroscopy (URS), percutaneous nephrolithotomy (PCNL) and extracorporeal shock wave lithotripsy (SWL), all of which are used in cystine stone management9,25–27 (Table 1).
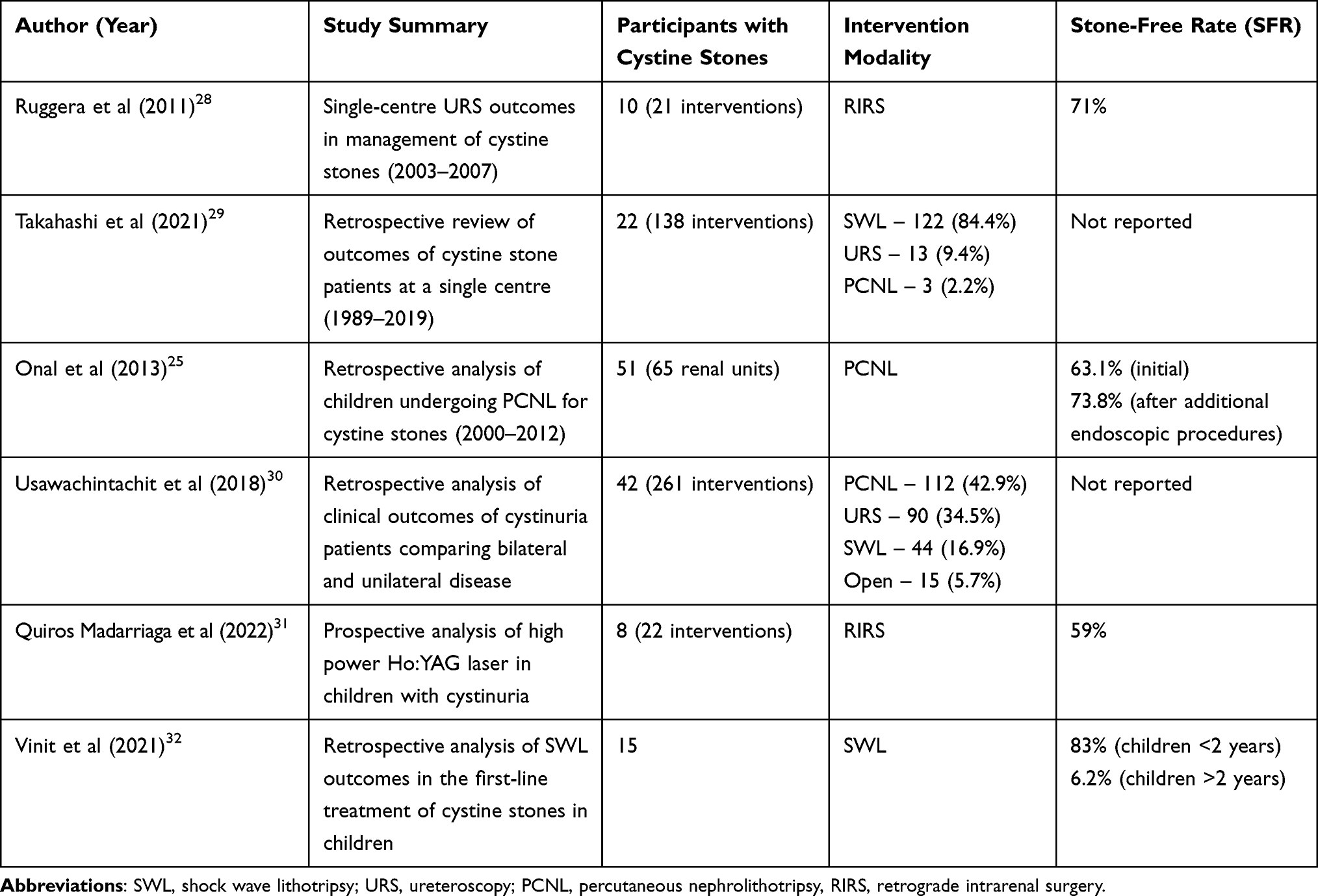 |
Table 1 Summary of Participants, Intervention Modalities and Outcomes of Selected Studies |
Although there are some disparities between the recommended management approaches of urinary stones depending on stone location and size by the AUA and EAU, they are relatively concordant, with URS or ESWL recommended for ureteric and renal stones <20 mm.19,20,27 Renal stones larger than 20 mm should be treated with PCNL. However, whilst the principles of these guidelines are applicable regardless of stone composition, specific consideration should be given to patients with cystine stones.
Shock wave Lithotripsy (SWL)
There is evidence to suggest that SWL may be less suitable for cystine stones compared with other stone types. Firstly, cystine stones can be relatively radiolucent and may be difficult to visualise on plain imaging, rendering targeting difficult in SWL.9 Furthermore, cystine stones may be more resistant to fragmentation by SWL than other types of stones and an increased number of shocks is required to achieve fragmentation than in a non-cystine stone.33 The AUA therefore recommend that cystinuric patients with ureteric stones that require definitive treatment should be offered ureteroscopy as a first-line treatment option.19
Studies have identified that cystine stones can be differentiated by their surface patterns being either smooth (cystine-S) or rough (cystine-R) with the latter having well-formed hexagonal crystalline structures that were more easily fragmented than smooth stones.34 Kim et al performed in vitro CT scanning of cystine stones, reporting that stones with a rough surface have lower attenuation values (702 vs 921 Hounsfield units) and have detectable internal radiolucent voids.35 Whilst this could theoretically assist in pre-operative decision making, in an in vivo study at a tertiary centre in which 107 cystinuric patients had CT imaging, it was not possible to distinguish between smooth and rough type cystine stones.36 There are also suggestions that cystine stones in patients taking thiol medications may be more susceptible to fragmentation.37
Studies have reported variable outcomes on efficacy of SWL in cystine stones. Cranidis et al reported a 54.5% success rate for renal stones with an average of 2.1 treatments/renal unit and had no success in treating ureteric stones with SWL.38 Conversely, Katz et al achieved successful stone clearance after two SWL treatments in 8 out of 10 patients with ureteric cystine stones and advocate this as a first-line treatment.39 Thomas et al report that 47% (15/32) of patients have stones responsive to SWL in which they consider first-line SWL in presence of previous success and a stone <1 cm.9 Kachel report that of 10 patients with cystine stones <1.5 cm, SWL was successful in achieving fragments of <3 mm in 60%, and <5 mm in 90%, however ureteric catheter or percutaneous nephrostomy was often used to administer contrast to help visualise the stones and it is not clear how many SWL treatments were required for each patient.37 SWL may have more of a role in paediatric cases of cystine stones, especially those younger than 2 years of age where stone-free rates of 83% were achieved in one study, however these were much lower in older children.32 Conversely, Landau et al reported a significantly lower 3-month SFR of 37.5% in children (mean age 6.6 years) with cystinuria compared with those without cystinuria (82.5%).40
Ureteroscopy and Cystine Stones
Ureteroscopy has seen substantial growth in recent years with a 257% increase in ureteroscopy over a 20-year period to 2020 in the UK.41 Technological advances with miniaturisation of endoscopic equipment, improved optical quality, disposable equipment, adjunctive tools (e.g. ureteric access sheaths, suction) and lasers have contributed to this increase.42 URS has been shown to be successful for both ureteric and renal cystine stones with Ruggera et al reporting a 71% SFR with a strict no residual fragments definition after initial URS for stones of a mean size of 11 mm, and in their series of 21 procedures, no major complications were reported.28 A systematic review of URS for managing large stones reported a SFR of 91% for a mean stone size of 2.7 cm, however a Clavien-Dindo ≥3 complication rate of 4.5% was noted.43 A recent consensus statement advocates the use of URS to manage renal and ureteral stones <20 mm to avoid more invasive PCNL in a patient group requiring frequent procedures, whilst also acknowledging that stones >20 mm may also be considered for treatment with staged ureteroscopic procedures.23 The risk of complications, particularly infective from URS and stone surgery increases with increased procedural time, and it has been recommended that procedural time is less than 90 minutes for this reason.44 Therefore, a staged procedure may prove a safer option in cases with a large stone burden in which ureteroscopic surgery is chosen.
Cystine stones commonly occur bilaterally in 67–73% of cases.29,30 Bilateral same-sitting ureteroscopy can be undertaken in the management of bilateral urolithiasis, and this is associated with an initial stone-free rate of 87%.45 Complication rates reported were 50%, although three-quarters of these were Clavien 1 complications.45 Complication rates reported in recent studies (2013–2016) are lower at 10.6%, and are lower in higher volume centres and in those where laser lithotripsy rather than pneumatic lithotripsy is performed.46
There has been an ever-increasing trend toward day case surgery for ureteroscopy over the last 5 years, with a 14.7% increase in day-surgery rates in the UK from 2015–2020 with a corresponding reduction in number of bed days and the associated costs.41 Day case surgery is still feasible in bilateral ureteroscopy, with rates of 60% reported in one study.47
Flexible URS has been successfully reported in the management of paediatric renal stones with a SFR of 87%.48 One small study of 22 procedures on 8 cystinuria patients, with a mean age of 9.3 years, reported a lower SFR of 59% as per ultrasound at one month and intraoperative complication rate of 18.2%.31
A challenge of flexible URS can be reaching the lower pole if there is a steep infundibulo-pelvic angle between the renal pelvis, limiting accessibility for laser lithotripsy of the stone, and requiring excessive deflection.49 Excessive deflection can risk damaging the ureteroscope with the laser fibre and if possible, the stone should be repositioned to the upper pole or renal pelvis with a basket to facilitate lasertripsy. Several single-use ureteroscopes are now available, which have a similar efficacy to reusable alternatives, but may be associated with increased costs.50 However, they have been shown to extend the life of reusable ureteroscopes by up to 40% and may be particularly useful in situations when risk of damage is higher including cystinuric patients with lower pole stones and large stone burdens.51
Ureteroscopy does have specific complications that should be considered, including ureteric strictures. A prospective study reported a post-ureteroscopy stricture incidence of 1.5% (4/263) and all of these were due to an impacted stone.52 A recent large-scale population-based study of >300,000 patients showed that overall stricture rate was 2.9% post ureteroscopy and the rates of stricture were 1.7-fold higher than for SWL, with instrumentation and stone-related factors increasing the risk.53 In one multi-centre study of 40 ureteric strictures, just 27.5% were managed endoscopically, with 37.5% requiring reconstruction, 25% required nephrectomy and 10% had chronic stent or nephrostomy.54 This would be particularly detrimental in cystinuria patients where CKD and nephrectomy rates are already high and urinary tract reconstruction would make any future interventions for recurrent cystine stones more challenging.
Decisions regarding inserting a ureteric stent post-ureteroscopy are made more challenging in cystinuric patients due to the increased risk of encrustation.23,55 When stents are inserted, it is recommended that they are in place for no more than two weeks to avert this risk.23,56 One tertiary centre advocates using stents on strings which can be removed by the patient in 1–3 days.9
Technological Advances in Ureteroscopy
Endourologists have an array of equipment available in their armamentarium including those that can be used to improve outcomes and individualise an approach to management of each patient.
Thulium fiber laser (TFL) is rapidly taking off in endourology as it has the advantages of a simpler cooling system enabling a smaller generator size, a smaller fibre diameter allowing increased irrigation and visibility, and lower pulse energy which results in reduced retropulsion compared with the Holmium:YAG laser.57 TFL can achieve a broader range of energy settings than a Ho:YAG laser, but ideal settings are not yet known and information regarding cost effectiveness is also currently lacking.57 When compared directly with Ho:YAG laser, while there are limited studies thus far investigating the role of TFL in managing cystine stones, an in vitro study has suggested effective dusting of cystine stone is possible.58
Ureteric access sheaths (UAS) have the advantage of facilitating multiple passages to the kidney with the flexible URS while reducing renal temperature and improving irrigation and therefore field of view, which may prove useful in cystinuric patients.59 Within the literature, there is an increased risk of mucosal damage to the ureters reported, especially if there is no pre-operative ureteric stent.60 There is conflicting evidence as to whether UAS increases the risk of ureteric strictures.59,61 However, with improvements in endourological technology with smaller diameter thulium laser fibres, irrigation through the ureteroscope alone may be adequate and may sway the balance of the risks and benefits against the use of UAS, but this will need to be considered on a case-by-case basis.62 The role of UAS in paediatric URS is also unclear and a recent systematic review showed a clear improvement in SFR and a 1.59% risk of ureteric injury requiring treatment with a stent.63
Irrigation fluid during ureteroscopy improves visualisation but can cause retropulsion of stones and an increase in intrarenal pressure (IRP). Increasing IRP beyond physiological parameters can increase pyelorenal backflow which is associated with an increased risk of infection.64 UAS can partially reduce IRP through improved drainage, but more recent technological advances have combined suction devices with UAS.59 Zhu et al compared outcomes of flexible URS for renal stones when using a 12/14F UAS with or without suctioning.65 They reported reduced operative time, lower urosepsis rates and higher initial SFRs for the suctioning UAS group, although SFRs at 3 months and septic shock incidence were comparable in both groups.
Yang et al have developed a novel “Postural Drainage Lithotripsy System” designed to increase passage of residual fragments using data from a CT urogram imaging.66 A spatial rotating bed is manipulating and moving the patient, using the CT derived data, to allow stone fragments to pass by gravity. In the preclinical study a stone in a 3D printed model was used with successful passage of stone fragment in 88% of cases. Although stone fragment clearance is vital in cystinuric patients, feasibility of achieving the angles of rotation in patients, cost and requirement for a CT urogram are potentially limiting factors to achieve this.
Percutaneous Nephrolithotomy (PCNL)
PCNL is the first-line recommended treatment option for renal stones >20 mm.27 PCNL however does have risks of haemorrhage requiring transfusion (up to 7%) and organ injury (0.4%) that can occur from calyceal puncture and tract dilatation.67 To mitigate these risks, there has been a trend for increasing miniaturisation of PCNL (mini-PCNL) instruments, which has been associated with comparable SFR to conventional PCNL with a lower blood loss but longer operative times.68 Porcine models have shown that there is less parenchymal damage caused by tracts 24 Fr or smaller, supporting the trend towards miniaturisation.69 Thus mini-PCNL may be of particular value in cystine stones where minimising the risk of complication is vital in a group requiring repeated interventions over their lifetime.23 In paediatric PCNL, Onal et al reported on their experience of PCNL in children with cystinuria, achieving an initial SFR of 63% using a combination of paediatric (<20 Fr) and adult (>20 Fr) access sheaths and a final SFR of 78% after an additional procedure (PCNL, URS or SWL).25 Blood transfusion was required in 12% of cases, however, all of these occurred in the >20 Fr access sheath group.
Although there may be concerns that PCNL can impair renal function due to the parenchymal damage caused by achieving access, a recent systematic review found this to not be the case and in three studies, there was a significant improvement in renal function following PCNL.70 However, the usage of multiple tracts during PCNL has been associated with a deterioration in renal function, particularly if pre-existing renal function is suboptimal.71,72 Consideration of endoscopic combined intrarenal surgery (ECIRS) should be given to those with large and complex stones to obviate the need for multiple tracts and this has been associated with increased one-step SFR, reduced need for additional procedures and a lower complication rate compared with PCNL but not mPCNL.73 Inoue et al reported on the benefits of miniaturised equipment, that could be used in the management of paediatric stones, in which a 2-year-old boy had bilateral renal stones >2 cm treated with a super ultra-mini ECIRS using a 8.5–9.5 Fr percutaneous tract sheath with a 6 Fr nephroscope.74
However, despite mini-PCNL offering reduced rates of complications, staged ureteroscopic procedures should be considered as an alternative and therefore large and complex cystine stones should be discussed in a stone multidisciplinary team meeting.9,10,75
Technological Adjuncts in PCNL
PCNL rates in cystinuric patients have remained relatively constant, due to the complexity of the stone burden and through miniaturisation of instruments reducing its complications.10 Ultrasound, pneumatic and laser techniques of lithotripsy are all used with PCNL. Newer technology such as the LithoClast Trilogy (EMS, Switzerland) combines ultrasonic and ballistic mechanisms with suction to increase stone clearance and also has favourable reviews on usability by surgeons.76 Shockpulse (Olympus, USA) technology also combines ballistic and pneumatic technology, with one study identifying reduced operative time and comparable SFR when compared with pneumatic lithotripsy.77 A further study suggested that Ho:YAG laser lithotripsy has higher SFR compared with pneumatic lithotripsy but comparable to Shockpulse lithotripsy.78 A systematic review of recent studies (2019 to 2021) has also shown that PCNL with laser lithotripsy achieved a SFR of 91.5% at 3 months.79 TFL has also recently been used in mini-PCNL achieving a SFR of 85% with reduced retropulsion, albeit for a relatively small mean stone size of 12.5 mm, and further comparative studies between Ho:YAG and TFL in PCNL laser lithotripsy are required.80
Fluoroscopic guidance has traditionally been used to achieve the percutaneous tract, but this has associated radiation exposure to both patients and surgeons, and the cumulative exposure to cystinuric patients must be considered as they are likely to undergo multiple procedures from a young age. A meta-analysis suggested that ultrasound and fluoroscopic guided PCNL had similar efficacy with respect to SFR and operative duration, and ultrasound guidance had a lower complication rate for Clavien I–II, but no difference for III–IV.81
Robotic Surgery
Open surgery is still occasionally used for complex cases, but it has been associated with kidney function deterioration in cystinuric patients, hence the need to seek alternatives where possible.82 There may be a growing role for robotic or laparoscopic surgery in cases where other minimally invasive techniques are not feasible.83 A systematic review comparing PCNL, robotic pyelolithotomy (RP) and laparoscopic pyelolithotomy (LP) reported similar outcomes for all modalities.84 However, there was a slightly lower SFR for PCNL compared with other modalities and PCNL had significantly higher blood loss, but this did not result in an increased transfusion rate. Varda et al performed four robotic lithotomy procedures on cystinuria patients, and the authors concluded that this offers a viable treatment option with reduced morbidity compared with open surgery when endoscopic surgery is not an option.85 Robotic surgery has been used in the management of paediatric urolithiasis, especially when there is concomitant ureteropelvic junction obstruction requiring pyeloplasty.86
The Avicenna Roboflex system (ELMED, Ankara, Turkey) is a robot-assisted flexible ureteroscopy system and Klein et al report a SFR of 90% in 240 patients using the system and cite a major advantage being the improved ergonomics offered to the surgeons, which is of importance in a long procedure when managing complex stones.87 Whilst the use of robot-assisted laparoscopic surgery for urolithiasis is likely to be restricted to the rare cases in which endoscopic surgery is not feasible, robot-assisted ureteroscopy may become more widely used in the future as the technology develops further.
Virtual Reality and Three-Dimensional Printing
Three-dimensional (3D) printing techniques can be used to produce models of an individual patient’s renal anatomy and stone positioning.88 3D printed models can also allow simulation PCNL, to allow for pre-procedural planning and to optimise target calyx for puncture in patients with complex stone burdens.89 Producing such models however requires specific equipment (3D printer) and is time-consuming and costly and this currently limits its uptake.
Virtual reality (VR) technology can be used to enhance surgical training by allowing trainees to develop practical skills in a simulated environment without risk to the patients.90 The Uro Mentor VR simulator for ureteroscopy is designed for training residents, with Cai et al reporting a significant improvement in procedure time, laser proficiency and total energy usage following a 4-hour training session.91 These technologies may be of greatest interest in PCNL which has a longer learning curve and selection of calyx for puncture is critical, to reduce the need for multiple punctures and the associated risks in cystinuric patients.88 Future studies should also take into account patient-reported outcome measures (PROMs) and nomograms to help achieve the best clinical outcomes.92,93
Conclusion
Cystine stones are rare and frequently recurrent, presenting a challenging patient cohort to manage. Whilst conservative and medical therapies to reduce stone formation in cystinuric patients are essential, there will inevitably be a need for surgical intervention in most patients. Due to the frequent need for intervention and its link with CKD, minimally invasive surgical techniques have much to offer. Shock wave lithotripsy, ureteroscopy and percutaneous nephrolithotomy all have a role, and technological advances in endourology are vital in achieving stone-free status and fragments entirely removed to prevent recurrences. The complexity of managing cystine stones necessitates a multidisciplinary team discussion, patient involvement and an individualised approach in a specialist centre for optimum management. Thulium fibre laser and virtual reality may have an increasing role in the future of cystine stone management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Lazaros Tzelves is a Research Associate of the European Association of Urology Guidelines Panel for Urolithiasis and Bladder Stones. Bhaskar Somani is a Member of the European Association of Urology Guidelines Urolithiasis Panel. The authors report no other conflicts of interest in this work.
References
1. Leusmann DB, Blaschke R, Schmandt W. Results of 5035 stone analyses: a contribution to epidemiology of urinary stone disease. Scand J Urol Nephrol. 1999;24(3):205–210. doi:10.3109/00365599009180859
2. Milliner DS, Murphy ME. Urolithiasis in pediatric patients. Mayo Clin Proc. 1993;68(3):241–248. doi:10.1016/S0025-6196(12)60043-3
3. Eggermann T, Venghaus A, Zerres K. Cystinuria: an inborn cause of urolithiasis. Orphanet J Rare Dis. 2012;7:19. doi:10.1186/1750-1172-7-19
4. Chillarón J, Font-Llitjós M, Fort J, et al. Pathophysiology and treatment of cystinuria. Nat Rev Nephrol. 2010;6:424–434. doi:10.1038/nrneph.2010.69
5. Wong KA, Mein R, Wass M, et al. The genetic diversity of cystinuria in a UK population of patients. BJU Int. 2015;116(1):109–116. doi:10.1111/bju.12894
6. Eisner BH, Goldfarb DS, Baum MA, et al. Evaluation and medical management of patients with cystine nephrolithiasis: a consensus statement. J Endourol. 2020;34(11):1103–1110. doi:10.1089/end.2019.0703
7. Rogers A, Kalakish S, Desai RA, Assimos DG. Management of cystinuria. Urol Clin North Am. 2007;34(3):347–362. doi:10.1016/j.ucl.2007.04.006
8. Sfoungaristos S, Hakim R, Katz R, et al. Cystine stones: a single tertiary center experience. J Endourol. 2015;29(3):362–366. doi:10.1089/end.2014.0478
9. Thomas K, Wong K, Withington J, Bultitude M, Doherty A. Cystinuria-a urologist’s perspective. Nat Rev Urol. 2014;11(5):270–277. doi:10.1038/nrurol.2014.51
10. Moore SL, Cook P, de Coninck V, et al. Outcomes and long-term follow-up of patients with cystine stones: a systematic review. Curr Urol Rep. 2019;20:27. doi:10.1007/s11934-019-0891-7
11. Streeper NM, Wertheim ML, Nakada SY, Penniston KL. Cystine stone formers have impaired health-related quality of life compared with noncystine stone formers: a case-referent study piloting the Wisconsin stone quality of life questionnaire among patients with cystine stones. J Endourol. 2017;31(S1):S48–S53. doi:10.1089/end.2016.0564
12. Prot-Bertoye C, Lebbah S, Daudon M, et al. CKD and its risk factors among patients with cystinuria. Clin J Am Soc Nephrol. 2015;10(5):842–851. doi:10.2215/CJN.06680714
13. Döven SS, Delibaş A, Taşkınlar H, Naycı A. The impact of surgical intervention on renal function in cystinuria. J Bras Nefrol. 2018;40(3):256–260. doi:10.1590/2175-8239-jbn-2018-0034
14. Matsunami M, Kinoshita K, Tanaka K, et al. Successful pre-emptive kidney transplantation in a cystinuria patient with nephrolithiasis-related end-stage renal disease. Ren Replace Ther. 2019;5:30. doi:10.1186/s41100-019-0226-7
15. Barbey F, Joly D, Rieu P, Méjean A, Daudon M, Jungers P. Medical treatment of cystinuria: critical reappraisal of long-term results. J Urol. 2000;163(5):1419–1423. doi:10.1016/S0022-5347(05)67633-1
16. Lindell A, Denneberg T, Edholm E, Jeppsson JO. The effect of sodium intake on cystinuria with and without tiopronin treatment. Nephron. 1995;71(4):407–415. doi:10.1159/000188760
17. Rodman JS, Blackburn P, Williams JJ, Brown A, Pospischil MA, Peterson CM. The effect of dietary protein on cystine excretion in patients with cystinuria. Clin Nephrol. 1984;22(6):273–278.
18. Königsberger E, Wang Z, Königsberger LC. Solubility of L-cystine in NaCl and artificial urine solutions. Monatshefte fuer Chemie. 2000;131:39–45. doi:10.1007/s007060050004
19. Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: American Urological Association/Endourological Society Guideline, part II. J Urol. 2016;196:1161. doi:10.1016/j.juro.2016.05.091
20. Geraghty RM, Davis NF, Tzelves L, et al. Best practice in interventional management of urolithiasis: an update from the European Association of Urology Guidelines Panel for Urolithiasis 2022. Eur Urol Focus. 2023;9(1):199–208. doi:10.1016/j.euf.2022.06.014
21. Reinstatler L, Stern K, Batter H, et al. Conversion from cystine to noncystine stones: incidence and associated factors. J Urol. 2018;200(6):1285–1289. doi:10.1016/j.juro.2018.07.047
22. Pak CY, Fuller CJ. Assessment of cystine solubility in urine and of heterogeneous nucleation. J Urol. 1983;129(5):1066–1070. doi:10.1016/S0022-5347(17)52543-4
23. Servais A, Thomas K, Dello Strologo L, et al. Cystinuria: clinical practice recommendation. Kidney Int. 2021;99(1):48–58. doi:10.1016/j.kint.2020.06.035
24. Moore SL, Somani BK, Cook P. Journey of a cystinuric patient with a long-term follow-up from a medical stone clinic: necessity to be SaFER (stone and fragments entirely removed). Urolithiasis. 2019;47(2):165–170. doi:10.1007/s00240-018-1059-5
25. Onal B, Dogan C, Citgez S, et al. Percutaneous nephrolithotomy in children with cystine stone: long-term outcomes from a single institution. J Urol. 2013;190(1):234–237. doi:10.1016/j.juro.2013.01.016
26. Trinchieri A, Montanari E, Zanetti G, Lizzano R. The impact of new technology in the treatment of cystine stones. Urol Res. 2007;35(3):129–132. doi:10.1007/s00240-007-0089-1
27. Hughes T, Ho HC, Pietropaolo A, Somani BK. Guideline of guidelines for kidney and bladder stones. Turk J Urol. 2020;46(Supp. 1):S104–S112. doi:10.5152/tud.2020.20315
28. Ruggera L, Zanin M, Beltrami P, Zattoni F. Retrograde transureteral approach: a safe and efficient treatment for recurrent cystine renal stones. Urol Res. 2011;39(5):411–415. doi:10.1007/s00240-010-0358-2
29. Takahashi T, Somiya S, Ito K, Kanno T, Higashi Y, Yamada H. The long-term follow-up of patients with cystine stones: a single-center experience for 13 years. J Clin Med. 2021;10(7):1336. doi:10.3390/jcm10071336
30. Usawachintachit M, Sherer B, Hudnall M, et al. Clinical outcomes for cystinuria patients with unilateral versus bilateral cystine stone disease. J Endourol. 2018;32(2):148–153. doi:10.1089/end.2017.0335
31. Quiroz Madarriaga Y, Badenes Gallardo A, Llorens de Knecht E, et al. Can cystinuria decrease the effectiveness of RIRS with high-power ho:yag laser in children? Outcomes from a tertiary endourology referral center. Urolithiasis. 2022;50(2):229–234. doi:10.1007/s00240-022-01301-w
32. Vinit N, Khoury A, Lopez P, et al. Extracorporeal shockwave lithotripsy for cystine stones in children: an observational, retrospective, single-center analysis. Front Pediatr. 2021;16(9):763317. doi:10.3389/fped.2021.763317
33. Williams JC, Saw KC, Paterson RF, Hatt EK, McAteer JA, Lingeman JE. Variability of renal stone fragility in shock wave lithotripsy. Urology. 2003;61(6):1092–1096. doi:10.1016/S0090-4295(03)00349-2
34. Bhatta KM, Prien EL, Dretler SP. Cystine calculi–rough and smooth: a new clinical distinction. J Urol. 1989;142(4):937–940. doi:10.1016/S0022-5347(17)38946-2
35. Kim SC, Hatt EK, Lingeman JE, Nadler RB, McAteer JA, Williams JC. Cystine: helical computerized tomography characterization of rough and smooth calculi in vitro. J Urol. 2005;174(4 Pt 1):1468–1470. doi:10.1097/01.ju.0000173636.19741.24
36. Warren H, Poon D, Srinivasan R, et al. Non-contrast computed tomography characteristics in a large cohort of cystinuria patients. World J Urol. 2021;39(7):2753–2757. doi:10.1007/s00345-020-03509-0
37. Kachel TA, Vijan SR, Dretler SP. Endourological experience with cystine calculi and a treatment algorithm. J Urol. 1991;145(1):25–28. doi:10.1016/S0022-5347(17)38237-X
38. Cranidis AI, Karayannis AA, Delakas DS, Livadas CE, Anezinis PE. Cystine stones: the efficacy of percutaneous and shock wave lithotripsy. Urol Int. 1996;56(3):180–183. doi:10.1159/000282836
39. Katz G, Kovalski N, Landau EH. Extracorporeal shock wave lithotripsy for treatment of ureterolithiasis in patients with cystinuria. Br J Urol. 1993;72(1):13–16. doi:10.1111/j.1464-410X.1993.tb06447.x
40. Landau EH, Shenfeld OZ, Pode D, et al. Extracorporeal shock wave lithotripsy in prepubertal children: 22-year experience at a single institution with a single lithotriptor. J Urol. 2009;182:1835–1839. doi:10.1016/j.juro.2009.04.084
41. Jour I, Lam A, Turney B. Urological stone disease: a 5-year update of stone management using Hospital Episode Statistics. BJU Int. 2022;130(3):364–369. doi:10.1111/bju.15728
42. Juliebø-Jones P, Keller EX, Haugland JN, et al. Advances in ureteroscopy: new technologies and current innovations in the era of Tailored Endourological Stone Treatment (TEST). J Clin Urol. 2022. doi:10.1177/20514158221115986
43. Geraghty R, Abourmarzouk O, Rai B, Biyani CS, Rukin NJ, Somani BK. Evidence for Ureterorenoscopy and Laser Fragmentation (URSL) for large renal stones in the modern era. Curr Urol Rep. 2015;16(8):54. doi:10.1007/s11934-015-0529-3
44. Lane J, Whitehurst L, Hameed BZ, et al. Correlation of operative time with outcomes of ureteroscopy and stone treatment: a systematic review of literature. Curr Urol Rep. 2020;21(4):17. doi:10.1007/s11934-020-0970-9
45. Rai BP, Ishii H, Jones P, Chapman RA, Stolzenburg JU, Somani BK. Bilateral simultaneous ureteroscopy for bilateral stone disease: a systematic review. Can J Urol. 2016;23(2):8220–8226.
46. Geraghty RM, Rai BP, Jones P, Somani BK. Bilateral Simultaneous Ureteroscopic (BS-URS) approach in the management of bilateral urolithiasis is a safe and effective strategy in the contemporary era-evidence from a systematic review. Curr Urol Rep. 2017;18(2):11. doi:10.1007/s11934-017-0660-4
47. Drake T, Ali A, Somani B. Feasibility and safety of bilateral same-session flexible ureteroscopy (FURS) for renal and ureteral stone disease. Cent Eur J Urol. 2015;68:193–196. doi:10.5173/ceju.2015.533
48. Whatley A, Jones P, Aboumarzouk O, Somani BK. Safety and efficacy of ureteroscopy and stone fragmentation for pediatric renal stones: a systematic review. Transl Androl Urol. 2019;8(Suppl 4):S442–S447. doi:10.21037/tau.2019.08.23
49. Mazzucchi E, Berto FCG, Denstedt J, et al. Treatment of renal lower pole stones: an update. Int Braz J Urol. 2022;48(1):165–174. doi:10.1590/s1677-5538.ibju.2020.1023
50. Talso M, Goumas IK, Kamphuis GM, et al. Reusable flexible ureterorenoscopes are more cost-effective than single-use scopes: results of a systematic review from PETRA Uro-group. Transl Androl Urol. 2019;8(Suppl 4):S418–S425. doi:10.21037/tau.2019.06.13
51. Ventimiglia E, Smyth N, Doizi S, et al. Can the introduction of single-use flexible ureteroscopes increase the longevity of reusable flexible ureteroscopes at a high volume centre? World J Urol. 2022;40:251–256. doi:10.1007/s00345-021-03808-0
52. Darwish AE, Gadelmoula MM, Abdelkawi IF, Abdellatif AM, Abdel-Moneim AM, Hammouda HM. Ureteral stricture after ureteroscopy for stones: a prospective study for the incidence and risk factors. Urol Ann. 2019;11(3):276–281. doi:10.4103/UA.UA_110_18
53. Sunaryo PL, May PC, Holt SK, Sorensen MD, Sweet RM, Harper JD. Ureteral strictures following ureteroscopy for kidney stone disease: a population-based assessment. J Urol. 2022;208(6):1268–1275. doi:10.1097/JU.0000000000002929
54. May PC, Hsi RS, Tran H, et al. The morbidity of ureteral strictures in patients with prior ureteroscopic stone surgery: multi-institutional outcomes. J Endourol. 2018;32(4):309–314. doi:10.1089/end.2017.0657
55. Andreassen KH, Pedersen KV, Osther SS, Jung HU, Lildal SK, Osther PJ. How should patients with cystine stone disease be evaluated and treated in the twenty-first century? Urolithiasis. 2016;44(1):65–76. doi:10.1007/s00240-015-0841-x
56. Clark CS, Gnanappiragasam S, Thomas K, Bultitude M. Cystinuria: an Overview of Challenges and Surgical Management. Front Surg. 2022;16(9):812226. doi:10.3389/fsurg.2022.812226
57. Schembri M, Sahu J, Aboumarzouk O, et al. Thulium fiber laser: the new kid on the block. Turk J Urol. 2020;46(Suppl 1):S1–S10. doi:10.5152/tud.2020.20093
58. Keller EX, De Coninck V, Doizi S, Daudon M, Traxer O. Thulium fiber laser: ready to dust all urinary stone composition types? World J Urol. 2021;39(6):1693–1698. doi:10.1007/s00345-020-03217-9
59. De Coninck V, Keller EX, Rodríguez-Monsalve M, Audouin M, Doizi S, Traxer O. Systematic review of ureteral access sheaths: facts and myths. BJU Int. 2018;122:959–969. doi:10.1111/bju.14389
60. Traxer O, Thomas A. Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol. 2013;189(2):580–584. doi:10.1016/j.juro.2012.08.197
61. Ulvik O, Harneshaug JR, Gjengsto P. Ureteral strictures following ureteroscopic stone treatment. J Endourol. 2021;35:985–990. doi:10.1089/end.2020.0421
62. De Coninck V, Somani B, Sener ET. Ureteral access sheaths and its use in the future: a comprehensive update based on a literature review. J Clin Med. 2022;11(17):5128. doi:10.3390/jcm11175128
63. Ripa F, Tokas T, Griffin S, et al. Role of pediatric ureteral access sheath and outcomes related to flexible ureteroscopy and laser stone fragmentation: a systematic review of literature. Eur Urol Open Sci. 2022;12(45):90–98. doi:10.1016/j.euros.2022.09.012
64. Tzelves L, Skolarikos A. Suction use during endourological procedures. Curr Urol Rep. 2020;21:46. doi:10.1007/s11934-020-00998-9
65. Zhu Z, Cui Y, Zeng F, Li Y, Chen Z, Hequn C. Comparison of suctioning and traditional ureteral access sheath during flexible ureteroscopy in the treatment of renal stones. World J Urol. 2019;37(5):921–929. doi:10.1007/s00345-018-2455-8
66. Yang T, Song R, Meng X, et al. A single center study that evaluates the preclinical use of a newly developed software and moving bed system to facilitate the spontaneous excretion of residual fragments after primary stone treatment (RIRS or PCNL). World J Urol. 2022;40(2):585–591. doi:10.1007/s00345-021-03863-7
67. Seitz C, Desai M, Häcker A, et al. Incidence, prevention, and management of complications following percutaneous nephrolitholapaxy. Eur Urol. 2012;61(1):146–158. doi:10.1016/j.eururo.2011.09.016
68. Ruhayel Y, Tepeler A, Dabestani S, et al. Tract sizes in miniaturized percutaneous nephrolithotomy: a systematic review from the European Association of Urology Urolithiasis Guidelines Panel. Eur Urol. 2017;72(2):220–235. doi:10.1016/j.eururo.2017.01.046
69. Emiliani E, Talso M, Baghdadi M, Traxer O. Renal parenchyma injury after percutaneous nephrolithotomy tract dilatations in pig and cadaveric kidney models. Cent Eur J Urol. 2017;70(1):69–75. doi:10.5173/ceju.2017.930
70. Reeves T, Pietropaolo A, Gadzhiev N, Seitz C, Somani BK. Role of Endourological Procedures (PCNL and URS) on renal function: a systematic review. Curr Urol Rep. 2020;21(5):21. doi:10.1007/s11934-020-00973-4
71. Hegarty NJ, Desai MM. Percutaneous nephrolithotomy requiring multiple tracts: comparison of morbidity with single-tract procedures. J Endourol. 2006;20(10):753–760. doi:10.1089/end.2006.20.753
72. Yadav R, Agarwal S, Sankhwar S, et al. A prospective study evaluating impact on renal function following percutaneous nephrolithotomy using Tc99m ethylenedicysteine renal scan: does multiplicity of access tracts play a role? Investig Clin Urol. 2019;60(1):21–28. doi:10.4111/icu.2019.60.1.21
73. Widyokirono DR, Kloping YP, Hidayatullah F, et al. Endoscopic combined intrarenal surgery vs percutaneous nephrolithotomy for large and complex renal stone: a systematic review and meta-analysis. J Endourol. 2022;36(7):865–876. doi:10.1089/end.2021.0761
74. Inoue T, Watanabe M, Shimada S, Kinoshita H, Matsuda T. Successful ultra-minimally invasive endoscopic intrarenal surgery for 2-year-old boy with bilateral cystine kidney stones over 2 cm. J Endourol Case Rep. 2018;4(1):101–104. doi:10.1089/cren.2018.0042
75. Barone B, Crocetto F, Vitale R, et al. Retrograde intra renal surgery versus percutaneous nephrolithotomy for renal stones >2 cm.A systematic review and meta-analysis. Minerva Urol Nefrol. 2020;72(4):441–450. doi:10.23736/S0393-2249.20.03721-2
76. Thakare N, Tanase F, Saeb-Parsy K, et al. Efficacy and safety of the EMS Swiss LithoClast® Trilogy for PCNL: results of the European multicentre prospective study on behalf of European Section of UroTechnology. World J Urol. 2021;39(11):4247–4253. doi:10.1007/s00345-021-03710-9
77. Yadav BK, Basnet RB, Shrestha A, et al. Comparison between shockpulse and pneumatic lithotripsy in percutaneous nephrolithotomy. World J Urol. 2021;39(3):915–919. doi:10.1007/s00345-020-03239-3
78. Rajeev TP, Pratihar SK, Sarma D, et al. A comparative study between holmium laser, pneumatic lithotripsy and shock pulse in terms of efficacy and safety in percutaneous nephrolithotomy (PCNL): a prospective randomized study. JELELU. 2020;3:e1–e8.
79. Rice P, Somani BK. Percutaneous laser nephrolithotripsy: is it here to stay? Results of a systematic review. Curr Opin Urol. 2022;32(2):185–191. doi:10.1097/MOU.0000000000000959
80. Enikeev D, Taratkin M, Klimov R, et al. Thulium-fiber laser for lithotripsy: first clinical experience in percutaneous nephrolithotomy. World J Urol. 2020;38:3069–3074. doi:10.1007/s00345-020-03134-x
81. Yang YH, Wen YC, Chen KC, Chen C. Ultrasound-guided versus fluoroscopy-guided percutaneous nephrolithotomy: a systematic review and meta-analysis. World J Urol. 2019;37(5):777–788. doi:10.1007/s00345-018-2443-z
82. Assimos DG, Leslie SW, Ng C, Streem SB, Hart LJ. The impact of cystinuria on renal function. J Urol. 2002;168(1):27–30. doi:10.1016/S0022-5347(05)64824-0
83. Suntharasivam T, Mukherjee A, Luk A, Aboumarzouk O, Somani B, Rai BP. The role of robotic surgery in the management of renal tract calculi. Transl Androl Urol. 2019;8(Suppl 4):S457–S460. doi:10.21037/tau.2019.04.06
84. Mantica G, Balzarini F, Chierigo F, et al. The fight between PCNL, laparoscopic and robotic pyelolithotomy: do we have a winner? A systematic review and meta-analysis. Minerva Urol Nephrol. 2022;74(2):169–177. doi:10.23736/S2724-6051.21.04587-0
85. Varda BK, Johnson EK, Johnson KL, Rosoklija I, Baum MA, Nelson CP. Imaging and surgical utilization for pediatric cystinuria patients: a single-institution cohort study. J Pediatr Urol. 2016;12(2):106.e1–7. doi:10.1016/j.jpurol.2015.08.019
86. Esposito C, Masieri L, Blanc T, Lendvay T, Escolino M. Robot-assisted laparoscopic surgery for treatment of urinary tract stones in children: report of a multicenter international experience. Urolithiasis. 2021;49(6):575–583. doi:10.1007/s00240-021-01271-5
87. Klein J, Charalampogiannis N, Fiedler M, Wakileh G, Gözen A, Rassweiler J. Analysis of performance factors in 240 consecutive cases of robot-assisted flexible ureteroscopic stone treatment. J Robot Surg. 2021;15(2):265–274. doi:10.1007/s11701-020-01103-5
88. De Sio M, Manfredi C, Fusco F, Creta M, Mirone V, Arcaniolo D. Recent advances in percutaneous lithotripsy techniques. Curr Opin Urol. 2021;31(1):24–28. doi:10.1097/MOU.0000000000000829
89. Xu Y, Yuan Y, Cai Y, et al. Use 3D printing technology to enhance stone free rate in single tract percutaneous nephrolithotomy for the treatment of staghorn stones. Urolithiasis. 2020;48(6):509–516. doi:10.1007/s00240-019-01164-8
90. Hameed BMZ, Somani S, Keller EX, et al. Application of virtual reality, augmented reality, and mixed reality in endourology and urolithiasis: an update by YAU Endourology and Urolithiasis Working Group. Front Surg. 2022;1(9):866946. doi:10.3389/fsurg.2022.866946
91. Cai JL, Zhang Y, Sun GF, Li NC, Yuan XL, Na YQ. Proficiency of virtual reality simulator training in flexible retrograde ureteroscopy renal stone management. Chin Med J. 2013;126(20):3940–3943.
92. Mehmi A, Jones P, Somani BK. current status and role of patient-reported outcome measures (PROMs) in Endourology. Urology. 2021;148:26–31. doi:10.1016/j.urology.2020.09.022
93. Jones P, Pietropaolo A, Chew BH, et al. Atlas of scoring systems, grading tools, and nomograms in endourology: a comprehensive overview from the TOWER Endourological Society Research Group. J Endourol. 2021;35(12):1863–1882. doi:10.1089/end.2021.0124